
Frans Radebe, NICD/NHLS
Krishnee Moodley, Chetna Govind and Nelesh P. Govender Adapted from a published case report (open-access publication under a creative commons license): Moodley K, et al. S Afr J HIV Med 2013;14:138-140.
A 46-year-old HIV-infected man on antiretroviral treatment was admitted to hospital with a history of fever and malaise. The patient had an undetectable HIV-1 viral load on admission with a CD4+ T-lymphocyte count of 435 cells/µl. He was also on haemodialysis for chronic renal disease (secondary to hypertension and diabetes mellitus), and had a central venous catheter (CVC) in situ. On examination, he was febrile and had evidence of severe mitral valve regurgitation with bilateral basal crackles. His admission total leucocyte count was elevated, i.e. 11.4 x 109 cells/l (reference range: 4.0 – 10.0 x 109 cells/l).
Question 1: What is your differential diagnosis and what investigations would you perform?
Answer to Q1
The differential diagnosis should include:
However, the diagnosis of IE fits best with the clinical history, examination and initial investigations. The aetiological causes of IE are numerous but broadly include bacterial and fungal pathogens. In order to confirm a diagnosis of IE, blood cultures and echocardiography should be performed immediately. Three sets of blood cultures should be obtained, preferably from different venepuncture sites and at different times (spaced at least 30 minutes apart).[1] This allows documentation of a continuous (rather than transient or intermittent) bloodstream infection which improves the specificity of an IE diagnosis. For adults, each blood culture bottle should contain at least 10 ml of blood to increase the yield. Prolonged incubation of blood cultures may be required for detection of fastidious or slow-growing pathogens (several weeks in some cases). In addition, a set of blood cultures obtained through the CVC could provide useful information. To minimise the chance of contamination of blood cultures, it is important to ensure proper skin antisepsis is performed before venepuncture; for blood obtained through the CVC, the port should first be disinfected with 70% alcohol. Other baseline investigations that would provide useful supporting evidence include a chest radiograph, full blood count with differential, C-reactive protein and serum 1,3 β-d glucan assay (this is helpful if a fungal cause of IE is likely because of the low sensitivity of blood cultures). The patient’s renal function would also need to be carefully monitored.
A single set of blood cultures cultured Candida parapsilosis.
The 1,3 β-d glucan levels were also markedly elevated (>523 pg/ml). Based on the pathogen identity and due to his impaired renal function, the patient was empirically started on intravenous fluconazole. On echocardiography, large, friable mitral valve vegetations were observed consistent with a diagnosis of fungal infective endocarditis (Figure 1). Blood cultures submitted 48 hours after commencing fluconazole, cultured the same organism.
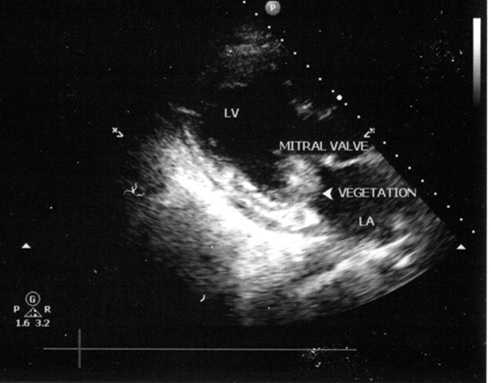
Figure 1: Echocardiography showing mitral valve vegetation (Moodley K, et al. S Afr J HIV Med 2013;14:138-140.)
Question 2: What are possible explanations for persistence of the organism in the bloodstream?
Answer to Q2
Low MICs were documented for this isolate and all tested antifungal agents including amphotericin B (no breakpoints), fluconazole (susceptible), voriconazole (susceptible) and caspofungin (susceptible). The haemodialysis CVC was removed and replaced. Culture of the CVC tip revealed C. parapsilosis with susceptibility results corresponding exactly to those of the blood culture isolate. The patient also underwent urgent mitral valve resection and replacement; excised valve tissue was submitted for microbiological and histological evaluation. An isolate identical to the admission blood culture and CVC tip culture was cultured from the valve tissue. Medical therapy with fluconazole was continued for six weeks. Blood cultures performed two weeks post-surgery were negative. However, repeat assays showed elevated 1,3 β-d glucan levels four weeks after therapy.
Question 3: What is the significance of a persistently elevated 1,3 β-d glucan assay in this clinical scenario?
Answer to Q3
1,3 β-d glucan, a cell wall component of many fungi, is detected by the Fungitell assay (Associates of Cape Cod Clinical Diagnostics, MA). The assay assists with early diagnosis of fungal bloodstream infections as it is often positive before traditional blood cultures. In one study, the 1,3 β-d glucan assay levels were found to be significantly higher in patients with C. parapsilosis, C. tropicalis and C. guilliermondii IE compared to those with Candida albicans endocarditis.[2]. In a meta-analysis published in 2011, the pooled sensitivity and specificity for diagnosis was 77% and 88% respectively.[3] This assay is also positive in patients with Pneumocystis pneumonia (PCP) but negative in patients with mucormycosis or cryptococcosis. β-D-glucan assay levels may be falsely elevated in patients with bacteraemia and in those on intravenous antibiotics (such as amoxicillin-clavulanic acid), immunoglobulin and haemodialysis where cellulose membranes have been utilized.[4]
The elevated follow-up 1,3 β-d glucan level in this patient was probably not clinically significant:
Question 4: What is the long-term management of this patient?
Answer to Q4
In this case, fluconazole was selected empirically and then continued, based on antimicrobial susceptibility results. Early aggressive surgical therapy combined with medical treatment resulted in a good outcome for the patient. Although combined medical and surgical therapy has decreased the mortality of patients with Candida IE, the mortality remains high. Long-term oral fluconazole therapy may be continued following intravenous therapy; however the duration of suppressive therapy is not clearly defined, with some patients requiring life-long therapy.[5]
In this patient, oral suppressive fluconazole therapy was continued. Two months following diagnosis, the patient remained clinically stable and continued with haemodialysis, fluconazole suppressive therapy and antiretroviral therapy.
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®