
Lyle Murray, MBChB, FCP (SA), MMed, DPhil
Jarrod Zamparini, MBChB, FCP (SA), MMed
Sarah Stacey, MBBCh, FCP (SA), Cert ID (SA), DTM&H
Jeremy Nel, MBChB, FCP (SA), Cert ID (SA), MMed, DTM&H
Division of Infectious Diseases, Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
Case presentation
A 36-year-old HIV-infected male presented to a Johannesburg hospital at the end of April 2021 complaining of worsening dyspnoea, chronic productive cough, fatigue, and nightsweats. He also had an eight-week history of skin rash on his face, neck, trunk, and limbs. He had been diagnosed with HIV two months prior to this presentation and initiated on a fixed-dose combination of tenofovir, lamivudine and dolutegravir and isoniazid prophylaxis at that time.
The skin lesions were not painful, were non-pruritic and were noted to have started prior to the initiation of the antiretrovirals and isoniazid. He had no history of prior chronic illness including tuberculosis.
On examination the patient appeared chronically ill with generalised wasting and shotty generalised, lymphadenopathy. His blood pressure was 118/76 mmHg, pulse 114 bpm, temperature of 37.8 °C and respiratory rate of 24 bpm.
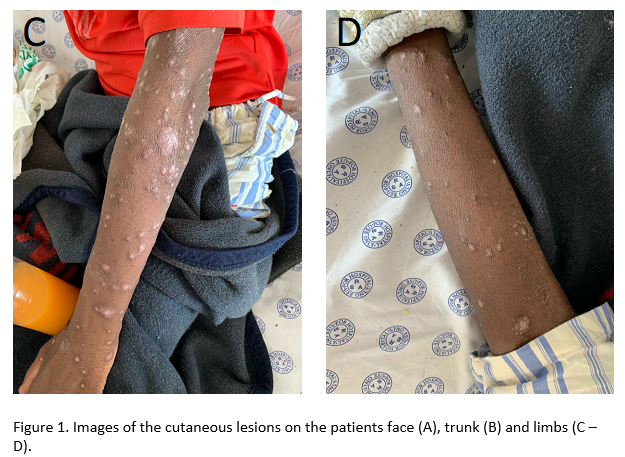
A dermatological examination revealed diffuse, erythematous, scaly papules with nodules and plaques over the face, neck, trunk and limbs (Figures 1 A-D). Some lesions were confluent. There was no mucous membrane involvement, and his hair was noted to be frail with diffuse alopecia. On auscultation of his chest he had bilateral crackles and his cardiovascular, abdominal and neurological examinations were unremarkable.
Images

Infectious differential diagnosis for the cutaneous manifestations
1. Disseminated mycosis
Disseminated mycoses in immunocompromised individuals frequently present with cutaneous manifestations as part of multisystem involvement1. In the South African context, particular mycoses to consider would include histoplasmosis, emergomycosis, cryptococcosis, sporotrichosis and blastomycosis. The morphology of cutaneous lesions is varied in mycoses and includes papules, nodules, ulcers, plaques and erythema2. Sporotrichosis typically presents with lymphocutaneous spread and cryptococcosis as skin-coloured papules or nodules. In this case the cutaneous manifestations are most suggestive of emergomycosis and histoplasmosis.
2. Disseminated tuberculosis with skin involvement
Cutaneous involvement
is a rare manifestation of extrapulmonary tuberculosis and may include papules,
warty lesions, ulcers and plaques3.The extensive nature of the skin involvement in this
case would indicate either haematogenous spread in the form of acute miliary
tuberculosis or papulonecrotic tuberculid. Papulonecrotic tuberculid, although
fitting morphologically in this case, is very unlikely in a patient with such
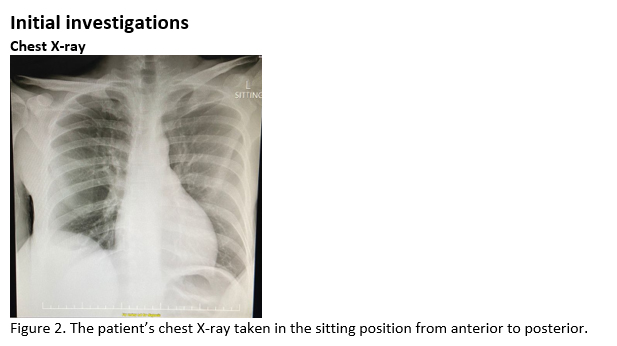
severe immune suppression. The chest x-ray features are also not suggestive of
miliary tuberculosis. A skin biopsy would be necessary to diagnose both of these
conditions.
3. Pruritic papular eruption (PPE) of HIV
PPE is the most common
rash associated with HIV infection and increases in frequency in individuals
with advanced immunosuppression, such as in this case4. Lesions are commonly papular, may progress to become
macular and nodular and are generally more confined to the extremities5. The lack of pruritis in this case combined with the
extensive distribution of the lesions argues strongly against a diagnosis of
PPE.
4. Syphilis
The rash of secondary syphilis can present in varied forms but is most commonly diffuse and symmetrical, involving macular or papular lesions on the trunk and extremities and frequently involves the palms and soles6. The rash is typically non-pruritic, and alopecia is common. A combination of treponemal and non-treponemal tests are required for the diagnosis.
Final diagnosis
1. Pulmonary tuberculosis (Rifampicin-sensitive)
2. Disseminated emergomycosis/histoplasmosis
Recommended reading
Samaddar, A. & Sharma, A. Emergomycosis, an Emerging Systemic Mycosis in Immunocompromised Patients: Current Trends and Future Prospects. Front. Med. 0, 550 (2021).
Schwartz, I. S. et al. AIDS-Related Endemic Mycoses in Western Cape, South Africa, and Clinical Mimics: A Cross-Sectional Study of Adults with Advanced HIV and Recent-Onset, Widespread Skin Lesions. Open Forum Infect. Dis. 4, 1–7 (2017).
Govender, N. P. & Grayson, W. Emergomycosis (Emergomyces africanus) in Advanced HIV
Disease. Dermatopathology 6, 63–69 (2019).
Oladele, R. O., Ayanlowo, O. O., Richardson, M. D. & Denning, D. W. Histoplasmosis in
Africa: An emerging or a neglected disease? PLoS Negl. Trop. Dis. 12, (2018).
PAHO and WHO. Guidelines for Diagnosing and Managing Disseminated Histoplasmosis among People Living with HIV. Guidelines for Diagnosing and Managing Disseminated Histoplasmosis among People Living with HIV (2020)
References
FIDSSA Members can earn CPD points by logging into the secure section of the website and visiting the MyCPD section.
Atlasville, Boksburg
South Africa
2022 © FIDSSA - All rights reserved • Website Terms of Use • Privacy Policy • Powered by E2
Admin login | Website login |
MYMEMBERSHIP®